
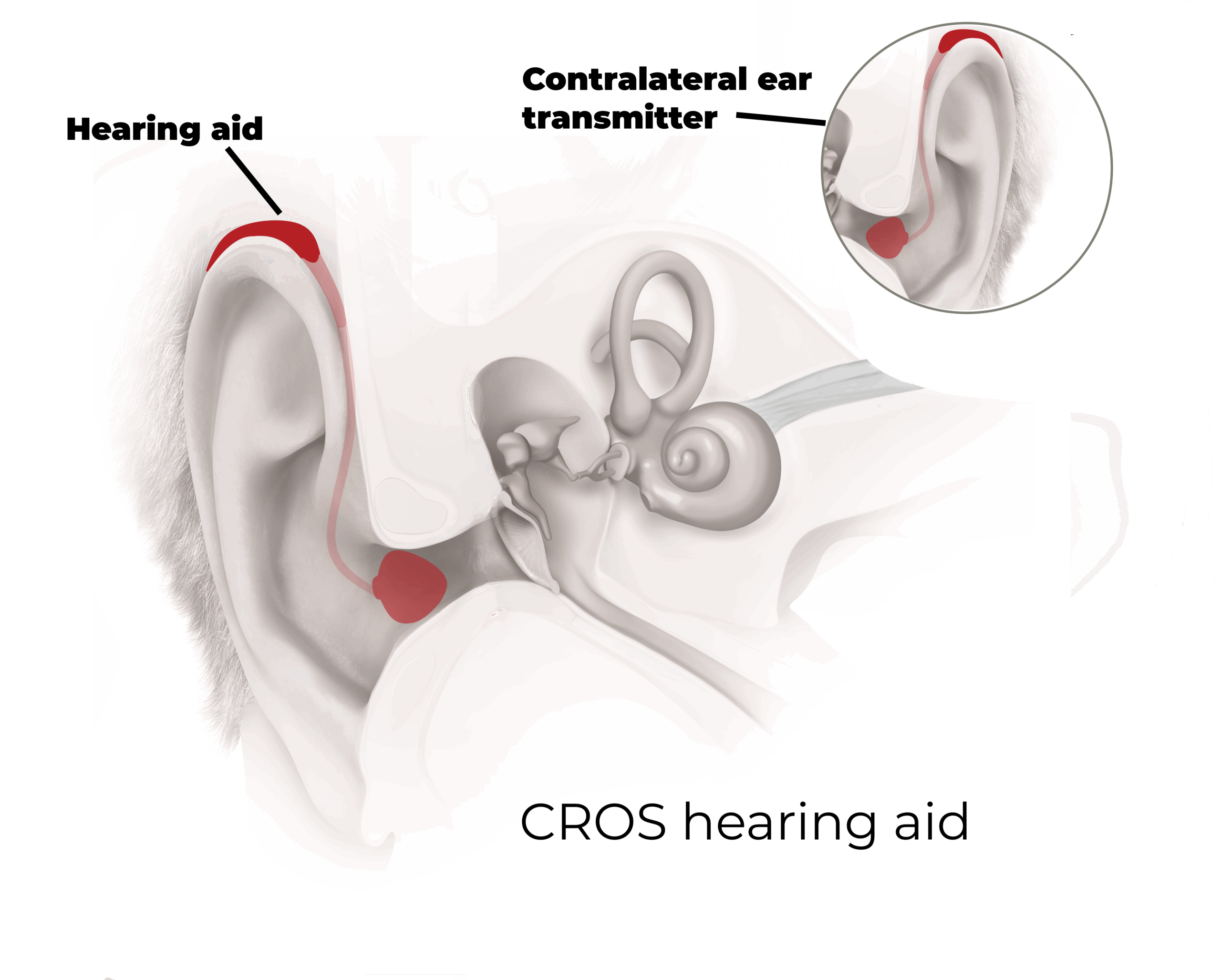
CROS Hearing Aids
This section outlines the benefits and drawbacks of CROS Hearing Aids, categorized into three key domains: audiological aspect, medical aspect, and patient-reported aspects.
Each publication listed below is rated by its importance for patients, using a Hearring key icon scale 🔑— one key for low importance, three keys for medium importance, and five keys for high importance.
🔑 low importance for patients
🔑🔑🔑🔑🔑the highest importance for patients
Benefits
Audiological Aspects
🔑🔑🔑
1. “CROS hearing aids transmit the sound from a microphone placed at the impaired ear to an amplifier and a receiver positioned at the normal ear. As there is no need for surgery, it is easily available in [unilateral sensorineural hearing loss] patients. ” (Ryu et al. 2014)
2. “BiCROS hearing aids also provide appropriate amplification for the functioning ear when the better ear has hearing loss. “
🔑🔑🔑🔑
1. “The primary benefit associated with the use of implantable or non-surgical cross-hearing devices is enhanced signal-to-noise ratio (SNR) in noisy and reverberant spaces, especially when the primary speech signal and background noise are spatially separated”
2. “The primary benefits realized from CROS hearing devices are improved sound awareness from the impaired side and better hearing in noise when speech is located at impaired side.”
More: Wazen et al. 2003, Hol et al. 2004, 2009, Niparko et al.2003, Finbow et al.
🔑🔑🔑🔑
1. (…) rerouting of signal does not result in restoration of binaural function, but serves to reduce the head-shadow effect.” (Snapp et al. 2017)
2. “As a result, lifting the negative effect of head shadow on monaural hearing as well as providing sound awareness of both sides of the head can be possible, and consequently enhancing spatial balance and speech perception ability in noise.” (Ryu et al. 2014)
Medical Aspects
🔑🔑🔑🔑
1. “… CROS hearing aids offer a nonsurgical option to compensate for some of the deficits that occur when a listener is limited to a single ear.” (Snapp 2019)
2. “The CROS system transmit sound signals from the impaired ear via a wire (or wireless) to a microphone in the better ear.
Compared to Cl, it is relatively inexpensive and non-invasive (
…)” (Cho et al. 2020)
3. To benefit from CROS hearing aids, no surgery is necessary and therefor in all situations the skin stays intact. (HEARRING consensus)
More: Bishop et al. 2010
🔑🔑🔑🔑
1. “As CROS hearing aids are a non-invasive solution, patients can easily try the device according to their needs. (HEARRING consensus)
🔑🔑🔑🔑
1. As CROS hearing aids are a non-invasive solution, only the removal of the device is necessary to undergo MRI. (HEARRING consensus)
Patient-reported Aspects
🔑🔑🔑
1. ” (…) noninvasive CROS solutions can successfully rehabilitate certain monaural listening deficits, provide improved hearing outcomes, and expand the reach of treatment in this population.” (Snapp et al. 2017)
More: Peters et al. 2015
Drawbacks
Audiological Aspects
🔑🔑🔑🔑
1. “(…) rerouting of signal does not result in restoration of binaural function, but serves to reduce the head-shadow effect.” (Snapp et al. 2017)
2. “The biggest limitation of CROS and BiCROS solutions is that binaural hearing is not restored. […] These devices cannot resolve an individual’s impairment for complex auditory tasks heavily reliant on binaural cues provided through binaural hearing, such as binaural summation, binaural squelch, or localization of sounds” (Snapp et al., 2019)
3. “The CROS and bone-anchored hearing aid treatment […] do not allow for real binaural hearing because the brain only receives and processes auditory input from one side.” (Arndt et al. 2011)
More: Bishop et al. 2010, Arndt et al. 2017, Peters et al. 2015
🔑🔑🔑
1. “Bone-anchored hearing aid (BAHA) or contralateral routing of signal (CROS) can improve the head shadow effect but do usually not reduce the perception of tinnitus. ” (Peter et al.2019)
2. “However, for people with severe to profound sensorineural hearing loss, hearing aids and other forms of sound enrichment are not useful for tinnitus treatment. In recent years, patients with severe to profound hearing loss have sought cochlear implantation as a means of tinnitus relief when other treatments were found to be ineffective.” (Holder et al. 2017)
🔑🔑🔑🔑
1. “There was no improvement in localization ability in the aided condition and no significant difference in performance with
CROS versus bone-anchored implants (BAI). ” (Snapp et al.2017)
2. “CROS solutions do not provide restoration of binaural hearing and cannot improve tasks requiring binaural input, such as localization.” (Snapp 2019)
More: Arndt et al. 2011, 2017, Cho et al. 2020, Augustine et al. 2012, Niparko et al. 2003, Hol et al. 2004, 2009, Peters et al. 2015
🔑🔑🔑🔑
1. “[Speech reception thresholds) were also impaired significantly by both [air conduction and bone conduction rerouting] device types when noise was presented toward the impaired ear. ” (Kitterick et al. 2016)
More: Arndt et al. 2011, 2017, Finbow et al. 2015, Snapp et al.2017
Medical Aspects
Patient-reported Aspects
🔑🔑🔑
1. “Most patients found it unpleasant to have an earmold with partial occlusion in their hearing ear (…)” (Müller-Isberner et al. 2015)